
Abstract:
Background: Globally 48% of children 0-6 months are exclusively breastfed. Breast milk contains bioactive components with anti-inflammatory properties that promote immune development. It contains antibodies and other immune factors, like white blood cells, that protects infants from infections, including respiratory illnesses. Undernutrition is estimated to be associated with 2.7 million child deaths yearly. Infant and young child feeding is highlighted as a factor to improve child survival and ensure healthy growth and development. In the first 2-years of life optimal nutrition can reduce morbidity including chronic diseases and mortality. South Africa remains the country with the lowest exclusive breastfeeding rates in Africa. Studies conducted in Low-middle-income-countries have shown that early initiation of breastfeeding and exclusive breastfeeding were protective against acute respiratory infections in children under-5 years. Despite the benefits of breastfeeding, Exclusive breastfeeding prevalence estimates remain low in LMICs (37%). There is evidence regarding suboptimal feeding practice and development of multiple infections in young children. Exclusive breastfeeding is known to protect against illnesses such as diarrhoea, gastro-enteritis, otitis media and respiratory tract infections such as bronchiolitis. Limited evidence for protection against TB in children. Considering the role of exclusive breastfeeding regarding immune properties, we hypothesis that using a longitudinal design, exclusive breastfeeding for the first 6-months can protect against TB and other respiratory infections. We will explore this association in children 0-13 years.
Methods: Data collection was nested in a prospective observational cohort study (Umoya) of children routinely presenting to a public hospital with respiratory symptoms presumptive of pulmonary tuberculosis (PTB). SPSS software was used for analysis and data was presented as frequencies to allow for descriptive study outcomes.
Results: A total of 490 children were recruited, with 438 presenting as symptomatic and 52 as healthy controls (no symptoms). Table 1 shows that gender was evenly distributed with a mean age of 2 years in the symptomatic group. More than 50% of the cohort had a caregiver who was employed or received a grant from the government as an income. 66% of participants resided in formal dwellings ie brick homes. 70% and 56% respectively were exclusively breastfed from the symptomatic and healthy control group. Only 45% of caregivers started their children on solids at 6-months. 339 Caregivers reported that they exclusively breastfed, however according to the WHO definition of exclusive breastfeeding, only 118 (24%) caregivers exclusive breastfed. 335 children presented with respiratory illness, including TB. Logistic regression showed that feeding type does not significantly predict TB-outcome.
Table 1: Demographic table describing the cohort
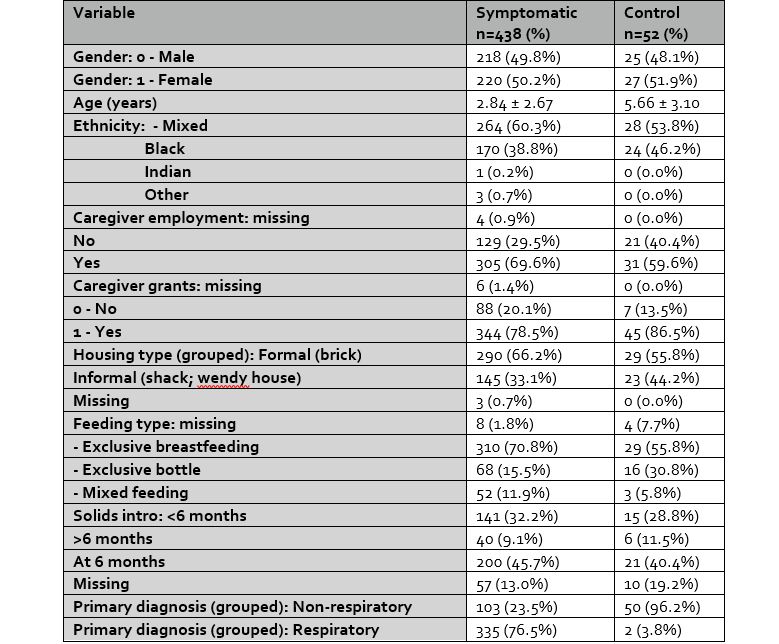
Conclusion: From this preliminary analysis, no significant association was found between feeding choice and TB outcome. This analysis provided a picture of the current infant feeding choices of caregivers within this population. The concept of exclusive breastfeeding continues to be misunderstood and requires ongoing advocacy and education. Further analysis within the cohort should continue to include role of early feeding and risk of TB, by considering contact information, growth and food security data.
Biography:
Mrs Margaret Van Niekerk is a early career colleague and is a registered PhD student working in Research at the Desmond Tutu TB Centre, at Stellenbosch university. She is a project manager who implements large observational studies in the field of paediatric infectious diseases. She holds a master’s degree in human nutrition and has a keen interest in Nutiriton in infectious diseases.
Copyright 2024 Mathews International LLC All Rights Reserved